The New York Times: Childbirth Is Deadlier for Black Families Even When They’re Rich, Expansive Study Finds
February 13, 2023 2:32 pmFor a wealthy country, the United States is a dangerous place to be a newborn. But it is not equally risky for all babies.
By Claire Cain Miller, Sarah Kliff, and Larry Buchanan / Feb 12, 2023
Produced by Larry Buchanan and Shannon Lin
In the United States, the richest mothers and their newborns are the most likely to survive the year after childbirth — except when the family is Black, according to a groundbreaking new study of two million California births. The richest Black mothers and their babies are twice as likely to die as the richest white mothers and their babies.
Research has repeatedly shown that Black mothers and babies have the worst childbirth outcomes in the United States. But this study is novel because it’s the first of its size to show how the risks of childbirth vary by both race and parental income, and how Black families, regardless of their socioeconomic status, are disproportionately affected.
“This is a landmark paper, and what it makes really stark is how we are leaving one group of people way behind,” said Atheendar Venkataramani, a University of Pennsylvania economist who studies racial health disparities and was not involved in the research.
The study, published last month by the National Bureau of Economic Research, includes nearly all the infants born to first-time mothers from 2007 to 2016 in California, the state with the most annual births. For the first time, it combines income tax data with birth, death and hospitalization records and demographic data from the Census Bureau and the Social Security Administration, while protecting identities.
That approach also reveals that premature infants born to poor parents are more likely to die than those born into the richest families. Yet there is one group that doesn’t gain the same protection from being rich, the study finds: Black mothers and babies.
“It suggests that the well-documented Black-white gap in infant and maternal health that’s been discussed a lot in recent years is not just explained by differences in economic circumstances,” said Maya Rossin-Slater, an economist studying health policy at Stanford and an author of the study. “It suggests it’s much more structural.”
If anything, the study’s findings understate the dangers of childbirth in much of the United States, a variety of researchers said, because California’s maternal mortality rate has been declining over the last decade, as deaths have gone up in the rest of the country.
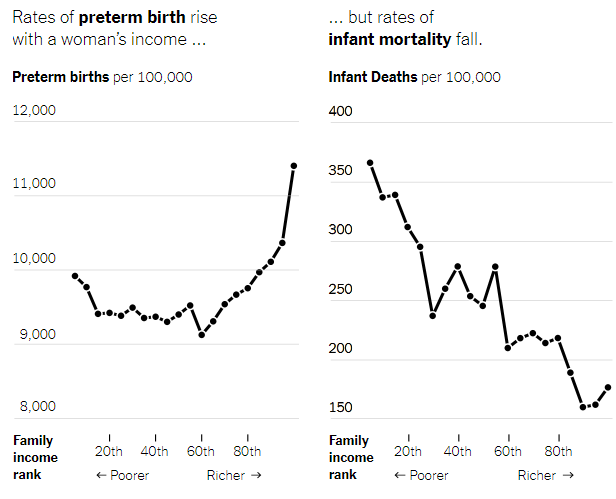
Rich Families Have More Premature Babies. But Those Babies Are Less Likely to Die.
Perhaps unexpectedly, babies born to the richest 20 percent of families are the least healthy, the study finds. They are more likely to be born premature and at a low birth weight, two key risk factors for medical complications early in life. This is because their mothers are more likely to be older and to have twins (which are more common with the use of fertility treatments), the researchers found.
But even with those early risk factors, these babies are the most likely to survive both their first month and first year of life.
A similar pattern emerged when it came to the health of the parents themselves: Rich and poor mothers were equally likely to have high-risk pregnancies, but the poor mothers were three times as likely to die — even within the same hospitals. Rich women’s pregnancies “are not only the riskiest, but also the most protected,” the paper’s authors wrote.
This finding suggests that the American medical system has the ability to save many of the lives of babies with early health risks, but that those benefits can be out of reach for low-income families.
Resources outside the medical system also play a role. Separate research on children with leukemia, for example, has found that even when treated at the same hospital and using the same protocol, those from high-income families fared better than those from poorer families.
“It’s not just about the medical care that kids are receiving,” said Anna Aizer, a health economist at Brown University. “There are all sorts of other things that go into having healthy babies. If you’re a higher-income mom who can take time off work, who doesn’t have to worry about paying rent, it’s not surprising you’ll be able to manage any health complications better.”
Money Protects White Mothers and Babies. It Doesn’t Protect Black Ones.
The researchers found that maternal mortality rates were just as high among the highest-income Black women as among low-income white women. Infant mortality rates between the two groups were also similar.
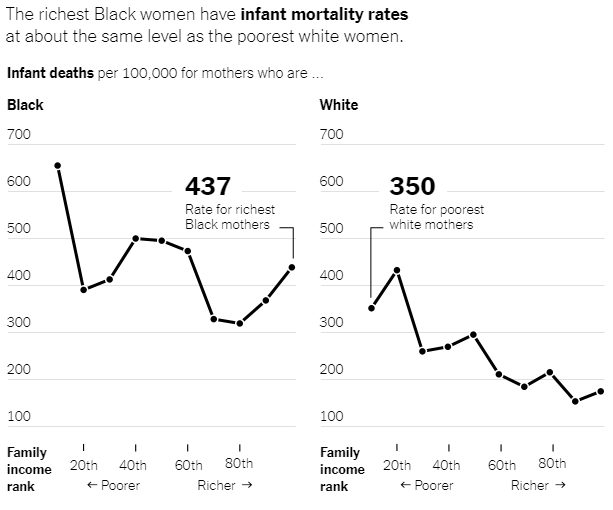
The babies born to the richest Black women (the top tenth of earners) tended to have more risk factors, including being born premature or underweight, than those born to the richest white mothers — and more than those born to the poorest white mothers. It’s evidence that the harm to Black mothers and their babies, regardless of socioeconomic status, begins before childbirth.
“As a Black infant, you’re starting off with worse health, even those born into these wealthy families,” said Sarah Miller, a health economist at the University of Michigan. She was an author of the study with Professor Rossin-Slater and Petra Persson of Stanford, Kate Kennedy-Moulton of Columbia, Laura Wherry of N.Y.U. and Gloria Aldana of the Census Bureau.
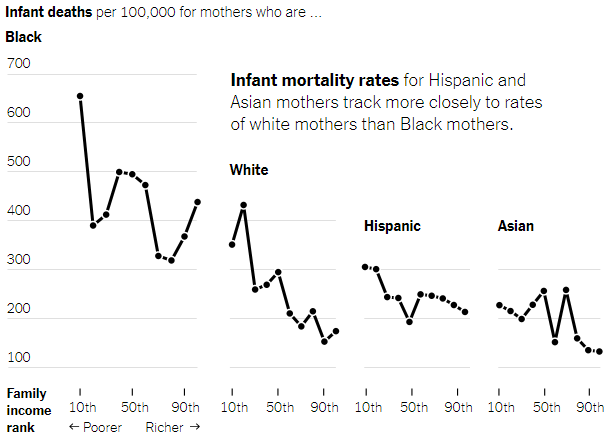
Black mothers and babies had worse outcomes than those who were Hispanic, Asian or white in all the health measures the researchers looked at: whether babies were born early or underweight; whether mothers had birth-related health problems like eclampsia or sepsis; and whether the babies and mothers died. There was not enough data to look at other populations, including Native Americans, but other research has shown that they face adverse outcomes nearing those of Black women and infants in childbirth.
Even before the new paper, research found that Black women with the most resources, as measured by education and class mobility, did not benefit during childbirth the way white women did. The new study demonstrates that disparities are not explained by income, age, marital status or country of birth. Rather, by showing that even rich Black mothers and babies have a disproportionately higher risk of death, the data suggests broader forces at play in the lives of Black mothers, Professor Rossin-Slater said.
“It’s not race, it’s racism,” said Tiffany L. Green, an economist focused on public health and obstetrics at the University of Wisconsin-Madison. “The data are quite clear that this isn’t about biology. This is about the environments where we live, where we work, where we play, where we sleep.”
There is clear evidence that Black patients experience racism in health care settings. In childbirth, mothers are treated differently and given different access to interventions. Black infants are more likely to survive if their doctors are Black. The experience of the tennis star Serena Williams — she had a pulmonary embolism after giving birth, yet said health care professionals did not address it at first — drew attention to how not even the most famous and wealthy Black women escape this pattern.
But this data shows how the effects of racism on childbirth start long before people arrive at the hospital, researchers across disciplines say, and continue after they leave. The stress of experiencing racism; air pollution in Black communities; and inequitable access to paid family leave, for example, have all been found to affect the health of mothers and babies.
“Even when it’s not about the direct disrespect that’s going on between the patient and the care provider, there are many ways systemic racism makes its way into the well-being of a pregnant or birthing person,” said Dr. Amanda P. Williams, the clinical innovation adviser at the California Maternal Quality Care Collaborative.
California Is a Best-Case Scenario. It Still Lags Behind Other Wealthy Parts of the World.
Many parts of the United States have much higher maternal mortality than California, and fewer policies to support families. California was the first state to offer paid family leave. It has one of the most generous public insurance programs for pregnant women. The state has invested in specific programs aimed at reducing maternal deaths and racial disparities in childbirth.
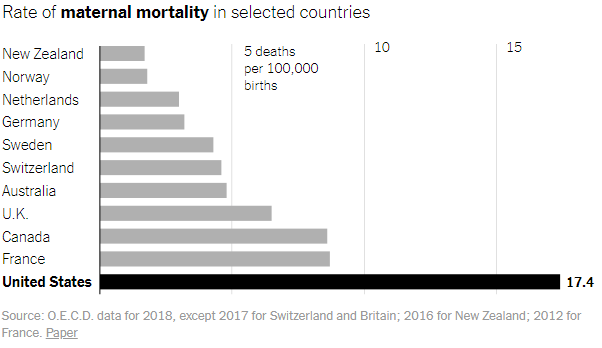
Yet even in this best-case American scenario, mothers and babies fare worse compared with another rich country the researchers examined: Sweden. At every income level, Swedish women have healthier babies. This held true for the highest-income Swedish women and those from disadvantaged populations, including low-income and immigrant mothers.
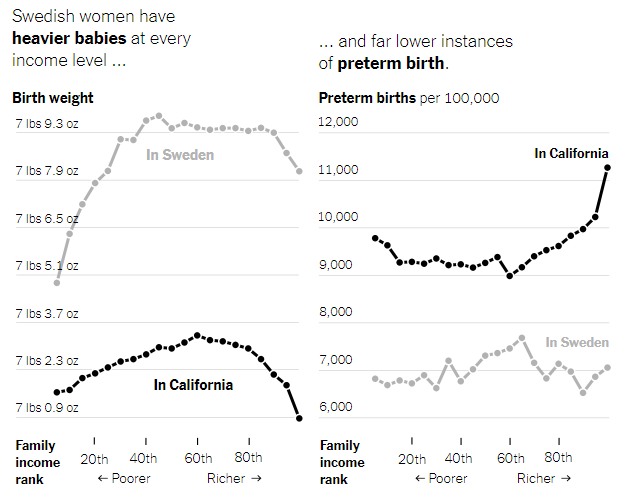
In the United States, earning more regularly translates into superior access to the fastest, most expensive health care. But even with that advantage, the richest white Californians in this study still gave birth to less healthy babies than the richest Swedish women. Their newborns were more likely to be premature or underweight. The two groups had roughly equal maternal death rates.
“That finding really does strongly suggest that it’s something about the care model,” said Dr. Neel Shah, chief medical officer of Maven Clinic for women’s and family health and a visiting scientist at Harvard Medical School. “We have the technology, but the model of prenatal care in the United States hasn’t really gotten an update in the last century.”
Sweden, like most European countries, has universal health insurance with low out-of-pocket costs for the patient. Midwives deliver most babies in Sweden and provide most of the prenatal care, which has been linked to lower C-section rates and lower rates of preterm births and low birth weights. It has long paid leaves and subsidized child care.
Like California, Sweden has also started targeted efforts to reduce maternal deaths. When officials there recognized that African immigrants giving birth were dying more frequently, they began piloting a “culture doula” program, with doulas who were immigrants themselves helping pregnant women navigate the country’s health system.
Local maternal health programs could begin to help reduce racial disparities in the United States, too, as could a more diverse medical workforce, research suggests. Nonprofits and universities have experimented with ways to address racism and poverty, with programs like cash transfers for low-income pregnant women and initiatives to improve the environments of Black communities.
By the time a woman is pregnant, Professor Miller said, “it’s almost too late.”
“Health is going to depend on exposures throughout her life, health care she’s received, environmental factors,” she said. “A lot goes on prior to the pregnancy that affects the health of the mother and baby.”
About the data
The researchers collected birth certificate data for all babies born to first-time mothers in California from 2007 to 2016. The final sample included 1.96 million births. They collected hospitalization and death records for babies for one year from the California Department of Health Care Access and Information, as well as hospitalization records for mothers for nine months before the birth and a year after. They collected maternal death records for the same period from a Social Security Administration data set. They provided birth records to the Census Bureau, which assigned anonymous identification codes to access I.R.S. data and determine new parents’ incomes in the two years before the birth. (Infant mortality records were available only until 2012. Maternal mortality data covers a longer period than in government records, which generally include data for six weeks after a birth, and most likely capture some deaths unrelated to childbirth.)
In Sweden, the researchers collected similar health and mortality data from the National Board of Health and Welfare. The final sample included 463,865 births. Analogous maternal morbidity data was unavailable. They linked babies to their parents and collected parents’ demographic and financial data from Statistics Sweden. Sweden has a smaller gap between the highest and lowest earners than the United States.
Read the original article in the New York Times